.jpg)
Cluneal Nerve Entrapment: A Frequently Missed Source of Buttock Pain
- Asian Pain Academy

- May 6
- 7 min read
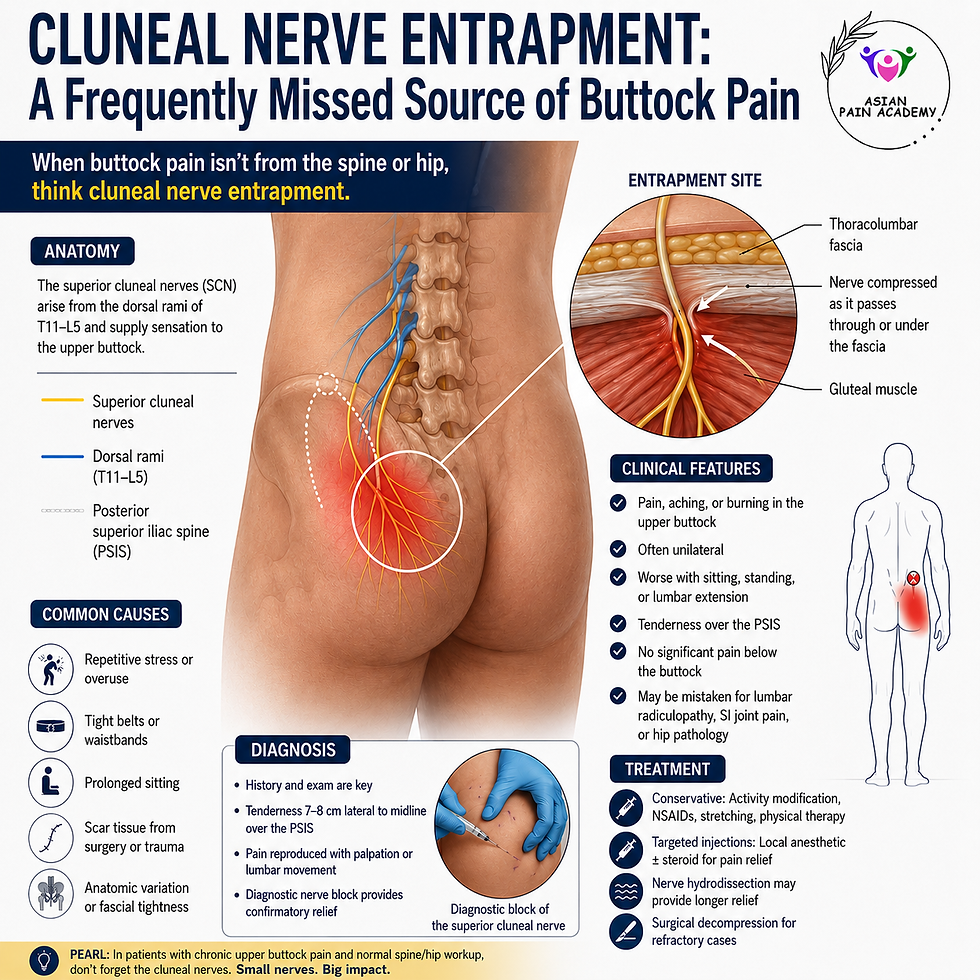
Buttock pain is a common yet diagnostically challenging complaint encountered in pain clinics, spine practices, and rehabilitation settings. While sacroiliac joint dysfunction, lumbar radiculopathy, piriformis syndrome, and facetogenic pain are frequently considered, cluneal nerve entrapment remains an under-recognized cause of chronic buttock and low back pain.
Failure to identify cluneal neuralgia can lead to prolonged suffering, unnecessary imaging, failed spine interventions, and even avoidable surgery. Increasing awareness among pain physicians and musculoskeletal clinicians is therefore essential. Modern ultrasound-guided diagnostic and therapeutic interventions now allow precise identification and treatment of this condition with excellent clinical outcomes.
What Are the Cluneal Nerves?
The cluneal nerves are purely sensory nerves supplying the skin over the gluteal region. They are divided into:
Superior cluneal nerves (SCN)
Middle cluneal nerves (MCN)
Inferior cluneal nerves (ICN)
Among these, superior cluneal nerve entrapment is the most commonly implicated in chronic buttock pain.
Superior Cluneal Nerves
The superior cluneal nerves arise from the dorsal rami of T11–L5 spinal nerves. They cross the posterior iliac crest through an osteofibrous tunnel formed by the thoracolumbar fascia and iliac crest. This region is the most common site of entrapment.
Middle Cluneal Nerves
The middle cluneal nerves originate from S1–S3 dorsal rami and traverse near the long posterior sacroiliac ligament, where they may become entrapped.
Why Is Cluneal Nerve Entrapment Commonly Missed?
Cluneal nerve entrapment frequently mimics:
Lumbar radiculopathy
Sacroiliac joint pain
Facet joint syndrome
Piriformis syndrome
Myofascial pain syndrome
Patients often undergo extensive lumbar imaging that may reveal incidental degenerative changes, diverting attention away from the true pain generator.
Importantly, MRI findings may appear minimal or unrelated despite significant symptoms.
Clinical Presentation
Patients typically describe:
Localized buttock pain over the posterior iliac crest
Burning or aching pain
Radiation into the lateral buttock or posterior thigh
Pain aggravated by standing, walking, lumbar extension, or prolonged sitting
Tenderness over the iliac crest, approximately 6–8 cm from the midline
Some patients report symptoms resembling sciatica despite the absence of true nerve root compression.
A characteristic finding is reproduction of symptoms on palpation over the entrapment point, sometimes associated with a Tinel-like sign.
Anatomy Relevant to Entrapment
The superior cluneal nerves penetrate the thoracolumbar fascia as they cross the iliac crest. Repetitive mechanical stress, fascial thickening, trauma, spinal degeneration, or postoperative fibrosis can compress the nerve at this osteofibrous tunnel.
Predisposing factors include:
Repetitive lumbar movements
Prior lumbar surgery
Trauma
Degenerative spine disease
Thoracolumbar fascial tightness
Athletes involved in rotational activities
Understanding this anatomy is critical during ultrasound-guided interventions.
Differential Diagnosis
Condition | Key Distinguishing Feature |
Lumbar radiculopathy | Dermatomal symptoms with neurological deficits |
Sacroiliac joint pain | Positive SI joint provocative tests |
Piriformis syndrome | Pain reproduced with FAIR test |
Facetogenic pain | Extension-rotation pain pattern |
Myofascial pain | Trigger points without neural distribution |
Failure to recognize cluneal nerve involvement may result in repeated unsuccessful epidural injections or spine surgery.
Clinical Examination
Important examination findings include:
1. Focal Tenderness
Tenderness over the posterior iliac crest, approximately 7 cm from midline, strongly suggests superior cluneal nerve entrapment.
2. Tinel-like Sign
Compression over the entrapment site may reproduce radiating buttock pain.
3. Sensory Changes
Some patients may exhibit localized dysesthesia or hyperesthesia over the gluteal region.
4. Absence of Neurological Deficit
Motor weakness and reflex changes are usually absent, helping differentiate from lumbar radiculopathy.
Role of Ultrasound in Diagnosis
Ultrasound has become increasingly valuable in identifying cluneal nerve entrapment and guiding interventions.
Benefits include:
Dynamic evaluation
Identification of fascial planes
Visualization of iliac crest anatomy
Real-time needle guidance
Avoidance of radiation
Improved procedural accuracy
Although direct visualization of small cluneal nerves may be challenging, anatomical landmarks permit reliable targeting.
Ultrasound-guided diagnostic blocks can confirm the diagnosis with high clinical utility.
Ultrasound Anatomy for Superior Cluneal Nerve Block
The patient is positioned prone with a pillow placed under the abdomen to reduce lumbar lordosis. A high-frequency linear ultrasound transducer is generally preferred.
The transducer is initially placed transversely over the posterior superior iliac spine and then moved laterally along the posterior iliac crest.
Important sonographic landmarks include:
Posterior iliac crest
Thoracolumbar fascia
Erector spinae muscles
Gluteus maximus muscle
Fascial crossing point over the iliac crest
The superior cluneal nerves typically traverse the osteofibrous tunnel approximately 6–8 cm lateral to the midline. Although the nerves themselves are often too small to visualize directly, the fascial tunnel and iliac crest serve as reliable procedural targets.
Ultrasound-Guided Superior Cluneal Nerve Block
Indications
Chronic buttock pain
Suspected superior cluneal neuralgia
Failed conservative management
Diagnostic confirmation
Therapeutic pain relief
Post-lumbar surgery buttock pain
Contraindications
Local infection
Uncorrected coagulopathy
Allergy to injectate
Patient refusal
Equipment Required
High-frequency linear transducer (10–15 MHz)
Sterile ultrasound gel and probe cover
22G–25G needle (50–80 mm depending on body habitus)
Local anesthetic
Corticosteroid if a therapeutic injection is planned
Skin antiseptic solution
Injectate Options
Diagnostic Block
Typical injectate:
2–5 mL of 0.25%–0.5% bupivacaine or ropivacaine
Therapeutic Block
Typical injectate:
Local anesthetic combined with a steroid
Example:
2 mL 0.25% bupivacaine
20–40 mg triamcinolone or equivalent corticosteroid
Hydrodissection using larger fluid volumes may be useful when fascial entrapment is suspected.
Step-by-Step Ultrasound-Guided Technique
Step 1: Patient Positioning
The patient is positioned prone with adequate exposure of the lower back and iliac crest region.
Step 2: Ultrasound Scanning
The transducer is placed transversely over the posterior iliac crest.
The iliac crest appears as a hyperechoic curved bony line with posterior acoustic shadowing.
The thoracolumbar fascia and overlying gluteal musculature are identified.
Step 3: Identification of Target Zone
The target region is usually located:
6–8 cm lateral to the midline
Along the posterior iliac crest
At the fascial crossing point of the superior cluneal nerve
Tenderness reproduction during probe pressure may further confirm the symptomatic site.
Step 4: Needle Insertion
An in-plane lateral-to-medial or medial-to-lateral approach may be used.
The needle is advanced under continuous ultrasound visualization toward the fascial plane overlying the iliac crest.
Step 5: Hydrodissection and Injection
After negative aspiration, a small amount of injectate is administered to confirm correct spread.
The injectate should separate the thoracolumbar fascia from the underlying tissues.
Successful hydrodissection often produces visible expansion of the fascial plane around the entrapment site.
Step 6: Post-Procedure Assessment
Immediate reduction in tenderness or buttock pain supports the diagnosis of superior cluneal neuralgia.
Patients are monitored briefly following the procedure.
Tips for Successful Ultrasound-Guided Cluneal Nerve Block
Always identify the posterior iliac crest first.
Scan dynamically along the crest to locate maximal tenderness.
Hydrodissection may improve outcomes in fascial entrapment.
Avoid excessively deep needle placement.
Real-time visualization improves safety and precision.
Reproduction of concordant pain during scanning is diagnostically valuable.
Potential Complications
Although generally safe, potential complications include:
Local pain
Bleeding
Infection
Steroid-related side effects
Incomplete pain relief
Temporary numbness
Ultrasound guidance significantly reduces procedural risk.
Advanced Interventional Options
In refractory cases, additional options include:
Pulsed radiofrequency treatment
Peripheral nerve stimulation
Surgical decompression
Repeated hydrodissection procedures
These interventions may be considered in carefully selected patients.
Clinical Pearls
Cluneal nerve entrapment should always be considered in patients with chronic buttock pain and normal lumbar imaging.
Focal tenderness over the posterior iliac crest is highly suggestive.
Superior cluneal neuralgia may mimic lumbar radiculopathy.
Diagnostic nerve blocks are both confirmatory and therapeutic.
Ultrasound guidance enhances safety and accuracy during interventions.
Hydrodissection can improve fascial release around the entrapped nerve.
Common Pitfalls
Mistaking Cluneal Neuralgia for Lumbar Disc Disease
Many patients undergo unnecessary spine procedures due to overlapping symptoms.
Inadequate Physical Examination
Failure to palpate the iliac crest region may lead to missed diagnosis.
Blind Injections
Landmark-guided injections may be inaccurate because of anatomical variability.
Frequently Asked Questions
What is cluneal nerve entrapment?
Cluneal nerve entrapment is compression or irritation of the cluneal nerves supplying the buttock region, leading to chronic buttock or low back pain.
Which cluneal nerve is most commonly affected?
The superior cluneal nerve is most commonly involved.
Can cluneal neuralgia mimic sciatica?
Yes. Many patients present with radiating buttock or posterior thigh pain resembling lumbar radiculopathy.
How is the diagnosis confirmed?
Diagnostic local anesthetic nerve blocks are commonly used to confirm the diagnosis.
Can ultrasound help in treatment?
Yes. Ultrasound guidance improves procedural precision, visualization of fascial planes, and injection accuracy.
Takeaways
Cluneal nerve entrapment is an underdiagnosed cause of chronic buttock pain.
Superior cluneal nerve involvement is most common.
Symptoms frequently mimic lumbar radiculopathy and sacroiliac joint pain.
Focal tenderness over the posterior iliac crest is an important clinical clue.
Ultrasound-guided diagnostic and therapeutic interventions are highly valuable.
Hydrodissection is increasingly used for fascial nerve entrapment syndromes.
Conclusion
Cluneal nerve entrapment is increasingly recognized as a significant yet frequently overlooked source of chronic buttock pain. Awareness of its anatomy, clinical presentation, and sonographic landmarks is essential for pain physicians, anesthesiologists, physiatrists, and musculoskeletal clinicians.
A focused clinical examination combined with ultrasound-guided diagnostic blocks can dramatically improve diagnostic accuracy and patient outcomes. As interventional pain medicine continues to evolve toward precision-based peripheral nerve interventions, recognition of cluneal neuralgia will become increasingly important in everyday clinical practice.
Learn More with Asian Pain Academy
Asian Pain Academy offers advanced training in:
Ultrasound-guided pain procedures
Interventional pain medicine
MSK ultrasound
Peripheral nerve interventions
Cadaveric workshops and live demonstrations
Explore fellowship programs and hands-on workshops designed for modern pain physicians and anesthesiologists.
About the Author – Dr. Debjyoti Dutta
Dr. Debjyoti Dutta is a renowned interventional pain physician and educator specializing in chronic pain management, musculoskeletal ultrasound, and image-guided pain procedures. He currently serves as a Consultant in Samobathi Pain Clinic.
He completed his MBBS with honours from Medical College Kolkata, followed by an MD in Anaesthesiology from King George's Medical University. He further pursued advanced fellowships in Pain Medicine and earned the prestigious FIPP (Fellow of Interventional Pain Practice) certification from the World Institute of Pain.
Dr. Dutta is actively involved in teaching and training physicians in ultrasound-guided and fluoroscopy-guided pain interventions through the Asian Pain Academy. He is a frequent national and international faculty speaker and has contributed extensively to pain medicine education, workshops, and scientific publications.
His areas of expertise include:
Chronic spine and joint pain
Ultrasound-guided pain interventions
Cancer pain management
Regenerative pain therapies
Neuropathic and musculoskeletal pain disorders
Dr. Debjyoti Dutta is also associated with several professional societies and has served in leadership roles within the Indian pain medicine community, contributing to academic research, guidelines, and physician training initiatives.



Comments