.jpg)
Nociplastic Pain: Redefining the Science of Chronic Pain
- Asian Pain Academy

- May 6
- 4 min read
Chronic pain has traditionally been classified into two major categories: nociceptive pain and neuropathic pain. While this framework has guided clinicians for decades, a significant number of patients continue to experience persistent pain that does not fit neatly into either category. These individuals often have widespread pain, fatigue, sensory hypersensitivity, sleep disturbances, and emotional distress despite minimal tissue injury or clear nerve damage.
To address this gap, the International Association for the Study of Pain (IASP) introduced a third mechanistic descriptor in 2017 — nociplastic pain. This concept has fundamentally changed how clinicians understand chronic pain syndromes and has opened new pathways for diagnosis and treatment.
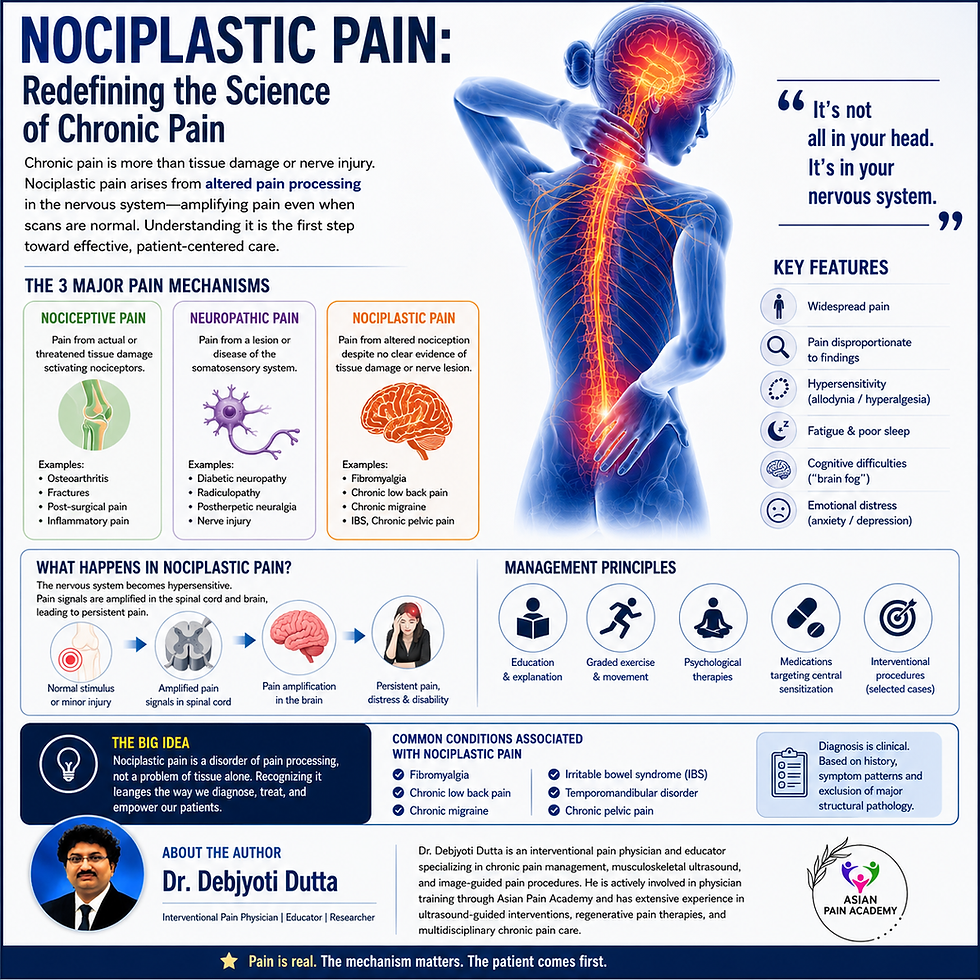
What Is Nociplastic Pain?
Nociplastic pain refers to:
“Pain that arises from altered nociception despite no clear evidence of actual or threatened tissue damage causing activation of peripheral nociceptors, or evidence for disease or lesion of the somatosensory system.”
In simpler terms, the nervous system becomes overly sensitive and amplifies pain signals even when there is no ongoing tissue injury or nerve damage.
Unlike nociceptive pain, where pain is driven by inflammation or structural pathology, or neuropathic pain, where pain results from nerve injury, nociplastic pain is primarily a disorder of pain processing.
Understanding the Three Major Pain Mechanisms
1. Nociceptive Pain
This occurs when pain receptors are activated due to tissue injury or inflammation.
Examples:
Osteoarthritis
Acute muscle strain
Postoperative pain
Fractures
The pain usually correlates with tissue damage and improves as healing occurs.
2. Neuropathic Pain
Neuropathic pain results from direct injury or disease affecting the nervous system.
Examples:
Diabetic neuropathy
Postherpetic neuralgia
Radiculopathy
Trigeminal neuralgia
Patients often describe burning, shooting, electric shock-like sensations.
3. Nociplastic Pain
Nociplastic pain occurs due to altered central pain processing and hypersensitization of the nervous system.
Examples:
Fibromyalgia
Irritable bowel syndrome
Chronic migraine
Temporomandibular disorder
Chronic pelvic pain
Chronic low back pain without clear pathology
In these conditions, imaging and laboratory investigations may appear normal or show findings insufficient to explain symptom severity.
Central Sensitization: The Core Mechanism
At the heart of nociplastic pain lies central sensitization — a state in which the central nervous system becomes hyperresponsive.
The spinal cord and brain essentially “turn up the volume” on pain signaling.
Patients may experience:
Pain from normally non-painful stimuli (allodynia)
Exaggerated pain responses (hyperalgesia)
Widespread pain distribution
Persistent pain after healing
Fatigue and cognitive dysfunction (“brain fog”)
Functional neuroimaging studies have demonstrated altered activity in pain-processing regions of the brain in patients with nociplastic disorders.
Why Nociplastic Pain Is Frequently Misunderstood
One of the greatest challenges in pain medicine is that nociplastic pain often lacks obvious structural abnormalities.
Patients are frequently told:
“Your MRI is normal.”
“Nothing is wrong.”
“It’s stress-related.”
“The pain is psychological.”
This misunderstanding can lead to:
Delayed diagnosis
Multiple unnecessary investigations
Inappropriate surgeries
Opioid overuse
Patient frustration and disability
Recognizing nociplastic pain validates the patient’s experience while shifting focus toward nervous system dysregulation rather than structural damage alone.
Clinical Features Suggestive of Nociplastic Pain
Certain patterns strongly suggest a nociplastic mechanism:
Key Characteristics
Widespread or diffuse pain
Symptoms disproportionate to imaging findings
Hypersensitivity to touch, sound, or light
Poor response to conventional analgesics
Associated fatigue and sleep disturbance
Cognitive dysfunction
Anxiety or depression coexistence
Multiple overlapping pain syndromes
Patients often report fluctuating symptoms influenced by stress, sleep quality, physical activity, and emotional state.
Common Conditions Associated with Nociplastic Pain
Fibromyalgia
Perhaps the prototypical nociplastic disorder, fibromyalgia is characterized by:
Widespread musculoskeletal pain
Fatigue
Sleep disturbance
Cognitive symptoms
There is increasing evidence of abnormal pain modulation and neurotransmitter imbalance.
Chronic Low Back Pain
Many patients with chronic low back pain have minimal imaging abnormalities despite severe symptoms. Central sensitization may explain persistent pain after tissue healing.
Chronic Migraine
Repeated migraine attacks may sensitize central pain pathways, transforming episodic headaches into chronic migraine syndromes.
Irritable Bowel Syndrome (IBS)
Visceral hypersensitivity and altered brain-gut interaction play a major role in IBS-related pain.
Diagnosis of Nociplastic Pain
There is no single laboratory test or imaging modality that confirms nociplastic pain.
Diagnosis relies on:
Clinical history
Symptom patterns
Pain distribution
Exclusion of major structural pathology
Identification of central sensitization features
Validated questionnaires such as the Central Sensitization Inventory (CSI) may aid assessment.
Treatment Principles
Managing nociplastic pain requires a multidimensional approach.
Purely structural treatments are often insufficient because the problem lies within altered pain processing.
Patient Education
Education itself is therapeutic.
Helping patients understand:
How pain processing changes occur
Why pain persists without ongoing injury
The role of the nervous system
can significantly reduce fear and catastrophization.
Exercise and Movement Therapy
Gradual, paced physical activity is among the most effective treatments.
Recommended approaches include:
Aerobic exercise
Strength training
Yoga
Tai chi
Aquatic therapy
Exercise helps normalize central pain modulation over time.
Psychological Therapies
Pain and emotion share overlapping neural networks.
Evidence-based approaches include:
Cognitive Behavioral Therapy (CBT)
Mindfulness-based stress reduction
Acceptance and Commitment Therapy (ACT)
These therapies improve coping, reduce fear avoidance, and decrease pain amplification.
Pharmacological Management
Certain medications target central sensitization mechanisms:
Commonly Used Medications
Duloxetine
Amitriptyline
Pregabalin
Gabapentin
Milnacipran
Traditional anti-inflammatory drugs may have limited effectiveness in purely nociplastic states.
Long-term opioid therapy is generally discouraged due to poor efficacy and risk of hyperalgesia.
Role of Interventional Pain Procedures
Interventional procedures may still have value when nociplastic pain overlaps with peripheral nociceptive generators.
Examples include:
Trigger point injections
Ultrasound-guided fascial plane injections
Neuromodulation
Peripheral nerve blocks
However, interventions should be integrated within a broader biopsychosocial treatment framework.
The Future of Pain Medicine
The recognition of nociplastic pain marks a major paradigm shift in medicine.
Pain is no longer viewed solely as a marker of tissue injury but as a complex output influenced by:
Neural processing
Emotional state
Sleep
Stress
Genetics
Environment
Future research may lead to:
Biomarkers for central sensitization
Precision pain medicine
Advanced neuromodulation techniques
Personalized rehabilitation strategies
Conclusion
Nociplastic pain has transformed the understanding of chronic pain disorders. By acknowledging altered nociception and central sensitization as legitimate biological mechanisms, clinicians can move beyond outdated structural models of pain.
For patients who have long suffered from persistent pain without clear answers, the concept of nociplastic pain provides validation, clarity, and a pathway toward more effective multidisciplinary care.
As pain medicine evolves, recognizing and addressing nociplastic mechanisms will become increasingly essential in improving outcomes for chronic pain patients worldwide.
About the Author
Dr. Debjyoti Dutta is an interventional pain physician and educator specializing in chronic pain management, musculoskeletal ultrasound, and image-guided pain procedures. He is actively involved in physician training through Asian Pain Academy and has extensive experience in ultrasound-guided interventions, regenerative pain therapies, and multidisciplinary chronic pain care.



Comments