.jpg)
Role of Glial Cells in Chronic Pain
- Asian Pain Academy

- May 6
- 11 min read

Core Concept - Role of Glial Cells in Chronic Pain
Chronic pain is no longer viewed as purely a neuronal phenomenon. Current neuroscience firmly establishes that glial cells — once dismissed as passive support cells — are active orchestrators of pain chronification, neuroinflammation, and central sensitisation. Understanding glial biology is essential to every modern clinician practising pain medicine.
Introduction: Why Pain Medicine Needed a New Paradigm
For decades, pain was understood through the lens of neurons — a linear chain of signals from damaged tissue to the brain. Yet the clinical reality confronted by pain physicians every day defies this simple model. Patients with chronic low back pain, fibromyalgia, complex regional pain syndrome (CRPS), and neuropathic pain continue to suffer even when the original structural lesion is resolved, when analgesics fail, and when imaging reveals nothing remarkable.
The explanation lies not in neurons alone, but in the cells that surround, nurture, and ultimately pathologically amplify them: glial cells. This paradigm shift — from a neuro-centric to a neuro-glial model of pain — is now one of the most important conceptual advances in modern pain medicine.
The International Association for the Study of Pain (IASP) defines chronic pain as pain persisting beyond normal tissue healing time, typically greater than three months. What this definition does not capture is the biological cascade that makes pain self-sustaining — a cascade driven largely by glial activation and neuroinflammation.
"Chronic pain is increasingly recognised as a condition of glia–neuronal dysregulation driven by persistent neuroinflammatory signalling."
What Are Glial Cells? A Clinical Overview
Glial cells outnumber neurons in the central nervous system (CNS). In fact, more than half of all cells in the CNS are glia — approximately 20–40% of which are astrocytes alone. They were historically considered mere "glue" (from the Greek glia), providing structural and metabolic support. This understanding has been radically revised.
Three glial subtypes are implicated in the genesis and maintenance of chronic pain:

Under physiological conditions, all three maintain homeostasis, support neuronal metabolism, regulate synaptic function, and provide anti-inflammatory neuroprotection. Under pathological conditions — nerve injury, tissue damage, persistent nociception — they undergo a dramatic transformation known as reactive gliosis or glial activation, amplifying pain signals while simultaneously losing their neuroprotective properties.
Microglia: The First Responders of Pain
Activation and the P2X4/TLR4 Cascade
Following peripheral nerve injury, primary afferent neurons become hyperexcitable and release signalling molecules — including ATP, the chemokine CX3CL1 (fractalkine), matrix metalloprotease-9 (MMP-9), and CCL2 (MCP-1) — into the spinal cord dorsal horn. These molecules bind to specific receptors on resident microglia, triggering their activation.
The critical intracellular event is phosphorylation of p38 MAPK (mitogen-activated protein kinase) in microglia, particularly via P2X4 receptor activation. This sets off a cascade that results in the synthesis and release of a potent cocktail of pain-amplifying mediators:


Sequential Glial Activation: Microglia First, Then Astrocytes
A critically important temporal distinction governs glial involvement in chronic pain. Nerve injury causes sequential activation of ERK — first in microglia (early phase) and then in astrocytes (late phase). This timing has profound clinical implications:
Hours to Days
Microglial Activation — Initiation Phase
P2X4 receptor activation, p38 MAPK phosphorylation, BDNF / IL-1β / TNF-α release. Microglia drive the development of acute-to-subacute pain hypersensitivity.
Days to Weeks
Astrocyte Activation — Amplification Phase
JNK activation in astrocytes; impaired glutamate clearance via EAAT2; elevated CXCL1 and CCL2. Astrocytes drive the maintenance of chronic pain states.
Weeks to Months
Sustained Neuroinflammation — Chronification
Glial mediators enter the CSF and cause remote central sensitisation beyond the original injury site — extra-territorial and widespread pain, as seen in nociplastic pain conditions.
Persistent State
Gliopathy — Loss of Neuroprotection
Reactive glia lose homeostatic, metabolic, and anti-inflammatory functions. The nervous system is now in a maladaptive, self-perpetuating pain state independent of peripheral input.
Astrocytes: The Architects of Chronic Pain Maintenance
If microglia light the fire, astrocytes ensure it keeps burning. As the most abundant cell type in the CNS, astrocytes are uniquely positioned to sustain chronic pain through multiple mechanisms operating simultaneously.
Impaired Glutamate Clearance via EAAT2
Under normal conditions, astrocytes rapidly remove glutamate from synapses via the excitatory amino acid transporter 2 (EAAT2), preventing excessive neuronal excitation. In reactive astrocytes, EAAT2 expression and function are significantly downregulated. The result is prolonged glutamate exposure at NMDA and AMPA receptors — a key driver of synaptic potentiation and central sensitisation. This mechanism directly contributes to the windup phenomenon experienced by pain physicians in clinical practice.
Connexin-43 Gap Junctions and Glial Synchronisation
A unique feature of astrocytes is their ability to directly communicate with each other through connexin-43 (Cx43) gap junction channels, freely exchanging ions and small cytosolic molecules. In chronic pain states, this gap-junction coupling becomes pathologically enhanced, allowing inflammatory signals to propagate across wide areas of the spinal cord — creating a "glial syncytium" that amplifies and sustains nociceptive signalling far beyond the original injury segment.
Metabolic Uncoupling from Neurons
Healthy astrocytes provide essential metabolic support to neurons — delivering lactate, maintaining ionic gradients, and buffering extracellular potassium. In reactive astrogliosis, this neuroprotective metabolic coupling is disrupted. Neurons are left metabolically vulnerable, with impaired energy support and increased susceptibility to excitotoxicity — further entrenching the chronic pain state.

Satellite Glial Cells: The Peripheral Pain Amplifiers
While most research has focused on CNS glia, the role of satellite glial cells (SGCs) in peripheral pain chronification is increasingly recognised as a critical and underappreciated mechanism. SGCs form a tight, complete cellular envelope around every sensory neuron soma in the dorsal root ganglia (DRG) and trigeminal ganglia. This intimate anatomical relationship places them in a uniquely powerful position to modulate peripheral nociceptor activity.
Normal SGC Function
In physiological conditions, SGCs maintain the microenvironment around sensory neurons — regulating ionic composition (particularly K⁺ buffering via Kir4.1 channels), providing metabolic support, and limiting the spread of neural signals between neighbouring neurons. They are essential gatekeepers of peripheral sensory neuron homeostasis.
SGC Activation After Nerve Injury
Following peripheral nerve injury, tissue inflammation, or diabetes-induced neuropathy, SGCs undergo dramatic morphological and molecular changes — most conspicuously, marked upregulation of GFAP (glial fibrillary acidic protein), the hallmark of reactive gliosis. This activation drives several pro-nociceptive consequences:
Connexin-43-mediated hyperexcitability: Activated SGCs markedly increase Cx43 expression, enhancing gap-junction coupling between SGC envelopes of adjacent sensory neurons. This creates electrical and chemical cross-talk between neurons that are normally isolated from one another — allowing a signal from one nociceptor to spread to neighbouring neurons, generating ectopic firing, hyperalgesia, and allodynia beyond the original injury territory.
CXCL1 upregulation: RNA sequencing studies in rat hyperalgesic priming models have demonstrated significant upregulation of CXCL1 in activated SGCs within the DRG — identifying CXCL1 as a key molecular mediator driving the transition from acute to chronic pain at the peripheral level.
Pro-inflammatory cytokine release: Activated SGCs release IL-1β, TNF-α, and ATP, which directly sensitise adjacent sensory neuron somata — lowering their activation threshold and contributing to peripheral sensitisation, a prerequisite for central sensitisation.

Glial Cells and the Biopsychosocial Model: A Neurobiological Bridge
The biopsychosocial model of pain has long recognised that psychological and social factors profoundly influence pain experience. Glial biology now provides the neurobiological mechanism that explains this relationship — bridging clinical observation with molecular neuroscience.
Stress, anxiety, depression, and sleep deprivation — all well-established pain modulators — directly activate microglial and astrocyte neuroinflammatory pathways. Glucocorticoids released under chronic stress, for example, paradoxically enhance microglial reactivity in chronic pain states. Conversely, social isolation has been shown in animal models to increase BDNF microglial signalling and worsen pain hypersensitivity.
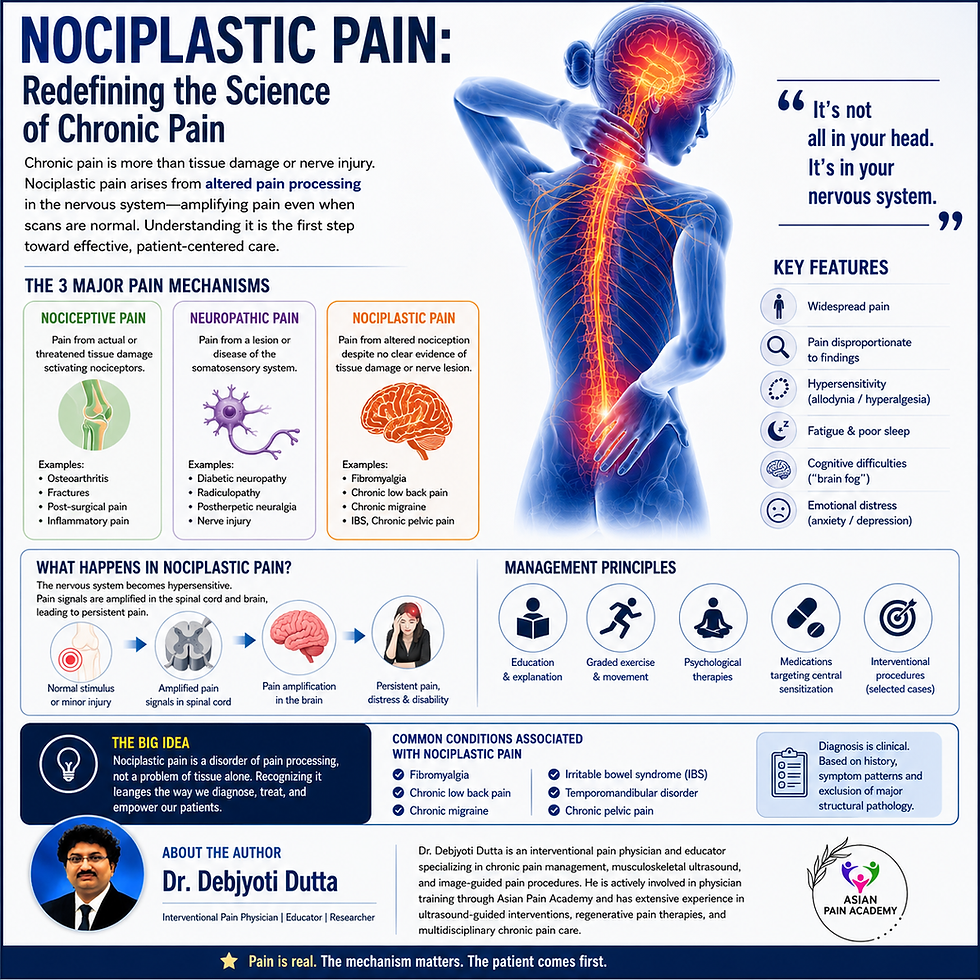
This is the neurobiological substrate of nociplastic pain — the IASP's third pain category (alongside nociceptive and neuropathic) — characterised by altered nociception arising from central sensitisation, often without clear peripheral pathology, and driven substantially by glial neuroinflammation. Conditions such as fibromyalgia, chronic widespread pain, and chronic primary pain represent clinical manifestations of this glially-mediated central dysregulation.
Sex Differences in Glial Pain Signalling: A Critical Emerging Area
One of the most important recent discoveries in glial pain biology is the identification of sexually dimorphic glial cell signalling. The mechanisms of microglial activation differ significantly between males and females, with profound clinical implications for pain management.
In male rodents, P2X4 receptor-driven microglial BDNF signalling is the dominant pathway for central sensitisation after nerve injury. In female rodents, T-lymphocytes appear to play a more significant role, with microglia less central to the process. Importantly, the specific mediators, kinetics, and pharmacological targets of glial pain signalling differ by sex — meaning that drugs targeting microglial pathways may show differential efficacy between male and female patients.
Given that chronic pain conditions — including fibromyalgia, migraine, and irritable bowel syndrome — disproportionately affect women, understanding sex-specific glial mechanisms is not an academic curiosity but a clinical imperative that will shape future pain therapeutics.
Is Chronic Pain a Gliopathy? Clinical Implications
Leading pain researchers, including seminal work published in Pain (Ji, Berta & Nedergaard, 2013), have proposed the concept of chronic pain as fundamentally a "gliopathy" — a disease of pathological glial activation, not merely neuronal dysfunction. This framing has profound clinical implications.
It explains why purely neuronal approaches — opioids, voltage-gated channel blockers, neuromodulators — provide incomplete relief in many chronic pain conditions. Neurons are being targeted, but the glial drivers of sensitisation continue unimpeded. It also explains the phenomenon of opioid-induced hyperalgesia: emerging evidence indicates that chronic opioid use itself activates microglia (via TLR4 signalling), progressively worsening central sensitisation and reducing analgesic efficacy over time — a vicious cycle with clear clinical relevance for pain physicians managing long-term opioid-dependent patients.

Therapeutic Strategies: Targeting Glial Cells in Chronic Pain Management
Understanding the glial basis of chronic pain opens new and exciting avenues for pain management — some already in clinical use, others still in the pipeline. This section presents the current therapeutic landscape through an interventional pain medicine lens.
Established and Emerging Pharmacological Targets
Minocycline (tetracycline-class antibiotic) is the most studied glial modulator in pain medicine. It inhibits microglial activation through multiple mechanisms: suppression of the NF-κB signalling pathway in activated glia, inhibition of inducible nitric oxide synthase (iNOS) and cyclooxygenase-2, reduction of oxidative stress through mitochondrial protection, and modulation of the MAPK pathway. In animal models, minocycline consistently attenuates the development of neuropathic pain and reverses antinociceptive tolerance to chronic morphine. Clinical translation has been variable, however, highlighting the complexity of translating glial targets from rodent models to human chronic pain.
Propentofylline, a glial modulator that inhibits microglial and astrocyte activation, showed remarkable efficacy in preclinical models across every animal model of clinical pain studied. However, clinical trials in humans with chronic pain did not reproduce these results — a sobering reminder that the complexity of long-standing human pain conditions exceeds current animal model fidelity. Research into dose optimisation and patient stratification continues.
P2X4 and TLR4 antagonists represent the most mechanistically precise targets identified in glial pain biology. Blocking the P2X4–p38 MAPK–BDNF axis or the TLR4-opioid interaction pathway could selectively inhibit microglial pain amplification without the broad systemic effects of current glial modulators.
Ceftriaxone, a beta-lactam antibiotic, upregulates EAAT2 expression in astrocytes — restoring impaired glutamate clearance and reducing central sensitization in preclinical models of neuropathic pain. It represents a pharmacological approach to targeting the astrocyte glutamate-reuptake deficit.
Non-Pharmacological Interventions with Glial Modulatory Effects
Several established interventional and rehabilitative approaches in pain medicine appear to exert therapeutic benefit, at least in part, through glial modulation. Spinal cord stimulation (SCS) has been shown in animal models to reduce microglial activation markers in the dorsal horn. Exercise therapy reduces spinal neuroinflammation and downregulates reactive astrogliosis. Cognitive-behavioural therapy (CBT) and mindfulness-based interventions modulate stress-hormone-driven microglial activation. These findings provide a neurobiological validation of the multimodal, biopsychosocial approach to chronic pain management that interventional pain physicians increasingly champion.
Neuromodulation and the Glial Hypothesis
Emerging evidence positions several neuromodulation targets — including DRG stimulation, high-frequency spinal cord stimulation, and transcranial magnetic stimulation — as having glial modulatory effects beyond purely neuronal mechanisms. Ketamine infusions, used in refractory complex regional pain syndrome, inhibit astrocyte NMDA receptors, reduce reactive astrogliosis, and normalise EAAT2 function. Lidocaine infusions may modulate TLR4-driven microglial activation. This mechanistic framework reinforces the rationale for interventional approaches in conditions driven by central sensitisation.
What This Means for the Modern Pain Physician: Clinical Pearls




Future Directions: The Frontier of Glial Pain Research
The field of glial pain biology is moving with remarkable speed toward clinically actionable insights. Several areas hold particular promise for the near future of chronic pain management:
Exosome therapy represents a novel approach to restoring homeostatic glial function. Mesenchymal stem cell-derived exosomes have shown the ability to shift microglial polarisation from pro-inflammatory M1 to anti-inflammatory M2 phenotypes in animal pain models — essentially re-educating activated glia toward their protective function.
Metabolic reprogramming of glia is emerging as a therapeutic strategy, targeting the disrupted energy metabolism in reactive astrocytes and microglia to restore neuroprotective function and reduce neuroinflammatory signalling.
Biomarkers of glial activation — including serum GFAP, neurofilament light chain (NfL), and CSF cytokine profiles — are being investigated as objective markers to stratify chronic pain patients by their degree of central neuroinflammation, enabling precision pain medicine approaches.
Single-cell RNA sequencing studies are revealing the remarkable heterogeneity of glial cell subtypes and their distinct contributions to different pain conditions — opening the door to highly targeted, cell-subtype-specific therapeutics.
Conclusion
The neuroscience of chronic pain has undergone a fundamental revolution. Glial cells — microglia, astrocytes, and satellite glial cells — are not bystanders in the pain experience. They are active, indispensable, and often dominant contributors to the initiation, amplification, and maintenance of chronic pain states.
For the interventional pain physician, this understanding transforms clinical reasoning. The patient with refractory neuropathic pain, the post-surgical pain syndrome that persists beyond healing, and the fibromyalgia patient dismissed by multiple specialists — all may be best understood through the lens of glial dysregulation and neuroinflammation. Their pain is real, it is neurobiologically grounded, and it requires therapies that address both the neuronal and the glial components of the pain matrix.
At the Asian Pain Academy, bridging this cutting-edge neuroscience with everyday clinical practice — from the consulting room to the ultrasound suite — is central to our mission. The clinician who understands glial biology is not only a better diagnostician but a more empathetic and effective pain healer.
Take Home Message

References & Further Reading
McKenzie A, Dombrower R, et al. Glial Activation, Neuroinflammation, and Loss of Neuroprotection in Chronic Pain: Cellular Mechanisms and Emerging Therapeutic Strategies. Biomedicines. 2025;14(1):58. doi:10.3390/biomedicines14010058
Ji R-R, Berta T, Nedergaard M. Glia and pain: Is chronic pain a gliopathy? Pain. 2013;154 Suppl 1:S10–28. PMC3858488
Ji R-R, Chamessian A, Zhang Y-Q. Pain regulation by non-neuronal cells and inflammation. Science. 2016;354(6312):572–577.
Cai W, et al. Central Nervous System Targets: Glial Cell Mechanisms in Chronic Pain. Neurotherapeutics. 2020. doi:10.1016/j.neurot.2020.08.012. PubMed:32820378
Lu HJ, Gao YJ. Astrocytes in Chronic Pain: Cellular and Molecular Mechanisms. Neurosci Bull. 2023;39(3):425–439. doi:10.1007/s12264-022-00961-3. PMC10043112
Ho YC, et al. Spinal microglia–neuron interactions in chronic pain. J Leukoc Biol. 2020;108(3):877–892. doi:10.1002/JLB.3MR0520-695R
Coull JAM, et al. BDNF from microglia causes the shift in neuronal anion gradient underlying neuropathic pain. Nature. 2005;438:1017–1021.
Trang T, et al. P2X4-receptor-mediated synthesis and release of brain-derived neurotrophic factor in microglia is dependent on calcium and p38-mitogen-activated protein kinase activation. J Neurosci. 2009;29(11):3518–28. PMC3759269
Ji R-R, et al. Neuroinflammation and central sensitization in chronic and widespread pain. Anesthesiology. 2018;129(2):343–366. PMC6051899
McGinnis A, Ji R-R. The Similar and Distinct Roles of Satellite Glial Cells and Spinal Astrocytes in Neuropathic Pain. Cells. 2023;12(6):965. doi:10.3390/cells12060965. PMC10047571
Du J, et al. Satellite glial cells drive the transition from acute to chronic pain in a rat model of hyperalgesic priming. Front Mol Neurosci. 2023;16:1089162. PMC9931746
Verkhratsky A, et al. Human glial cells as innovative targets for the therapy of central nervous system pathologies. Cells. 2024;13(7):625. PMC11011741
Zychowska M, et al. Glial Modulator Antibiotics for Neuropathic Pain: Current Insights and Future Directions. Pharmaceuticals. 2025;18(3):346. doi:10.3390/ph18030346. PMC11944926
Watkins LR, Maier SF. GLIA: A novel drug discovery target for clinical pain. Nat Rev Drug Discov. 2003;2(12):973–985. doi:10.1038/nrd1251
Raghavendra V, et al. Role of microglia in neuropathic pain, postoperative pain, and morphine tolerance. J Neuroimmunol. 2003;185:11–15. PMC3169792
Dr Debjyoti Dutta, author - Role of Glial Cells in Chronic Pain
Interventional Pain Physician · Educator · Researcher | Founder, Asian Pain Academy
Dr Debjyoti Dutta is a specialist in interventional pain medicine with expertise in ultrasound-guided procedures, chronic pain management, and neuromodulation. As the founder of the Asian Pain Academy, he is dedicated to advancing evidence-based pain education for physicians and healthcare professionals across Asia. His clinical and academic work bridges modern pain neuroscience — including glial biology and nociplastic pain — with practical, patient-centred interventional approaches.


Comments